
Dd Form 2870 - The attached dd form 2870, authorization for disclosure of medical or dental information, authorizes fox army health center (fach) to release medical information.
Dd Form 2870 - Patient date of birth 3. Full name in (last, first, middle initial) format. Please fill out the authorization for disclosure of medical or dental. Short requests (less than 50 pages) can be. Find and fill out the correct.
Date of birth in (yyyymmdd) format. Web authorization for disclosure of medical or dental information dd form 2870, dec 2003 adobe professional 8.0 Web the attached od form 2870, authorization for disclosure of medical or dental information, serves as the mechanism for beneficiaries to request copies of their medical record. On any device & os. Web (dd form 2870) this form is used to allow a tricare beneficiary to authorize health net federal services, llc (health net) to release protected information. Try it for free now! Web use signnow to design and send out dd form 2870 for collecting signatures.

Dd Form 2870 Printable Printable Templates
Web instructions for filling out dd form 2870 (authorization for disclosure of medical or dental information) 1. Web (dd form 2870) this form is used to allow a tricare beneficiary to authorize health net federal services, llc (health net) to release protected information. Web the attached dd form 2870, authorization for disclosure of medical or.

DD 1840R 19882021 Fill and Sign Printable Template Online US Legal
Date of birth in (yyyymmdd) format. Patient’s date of birth block 3: Web dd form 2870 general instructions this form is used to allow an applicant to authorize the release of protected information to a person or entity of the beneficiary’s. Web instructions for filling out dd form 2870 (authorization for disclosure of medical or.

Dd Form 2870 Printable Printable Templates
Da form 3365, da form 3443, da form 3443x, da form 3443y, da form 3443z, da. Web (dd form 2870) this form is used to allow a tricare beneficiary to authorize health net federal services, llc (health net) to release protected information. Web to complete the dd form 2870, please follow the below instructions: Web.

Dd Form 2870 Fill Online, Printable, Fillable, Blank pdfFiller
Upload, modify or create forms. Da form 3365, da form 3443, da form 3443x, da form 3443y, da form 3443z, da. Authorization for disclosure of medical or dental. On any device & os. Web the attached dd form 2870, authorization for disclosure of medical or dental information, authorizes reynolds army health clinic (rach)to release medical.

Dd form 2870 Blank 9 Best S Of Dd form 2745 Blank Blank Da form 4002
Upload, modify or create forms. Be ready to get more. _____ mental health clinical records _____ hiv/aids related information. Patient date of birth 3. Web submit the completed dd form 2870 to the relevant military hospitals or clinics. Web requests for medical records by patients require a filled out and signed dd form 2870 and.

Dd Form 2870 Printable Improve your tax management airSlate
Web (dd form 2870) this form is used to allow a tricare beneficiary to authorize health net federal services, llc (health net) to release protected information. Short requests (less than 50 pages) can be. Web instructions for filling out dd form 2870 (authorization for disclosure of medical or dental information) 1. Be ready to get.

DD Form 2870 Printable Dd Form 2870 blank, sign online — PDFliner
Web provide release of information form dd form 2870 dod identification card complete all highlighted section on dd form 2870 provide current telephone number and address. _____ mental health clinical records _____ hiv/aids related information. Be ready to get more. Web dd form 2870, dec 2003 prescribed by: Patient’s date of birth block 3: Short.

2023 Form DD 2870Fill Online, Printable, Fillable, Blank pdfFiller
Please fill out the authorization for disclosure of medical or dental. Edit, sign and save dd 2870, dec form. Authorization for disclosure of medical or dental information (dd form 2870) your provider or contractor will use this form is to get your permission to. Web requests for medical records by patients require a filled out.

Dd 2870 Army Pubs Army Military
Create this form in 5 minutes or less. Date of birth in (yyyymmdd) format. Web iach form 2870 (2023) for the following to be included, initial below to authorize disclosure: The attached dd form 2870, authorization for disclosure of medical or dental information, authorizes fox army health center (fach) to release medical information. Web to.
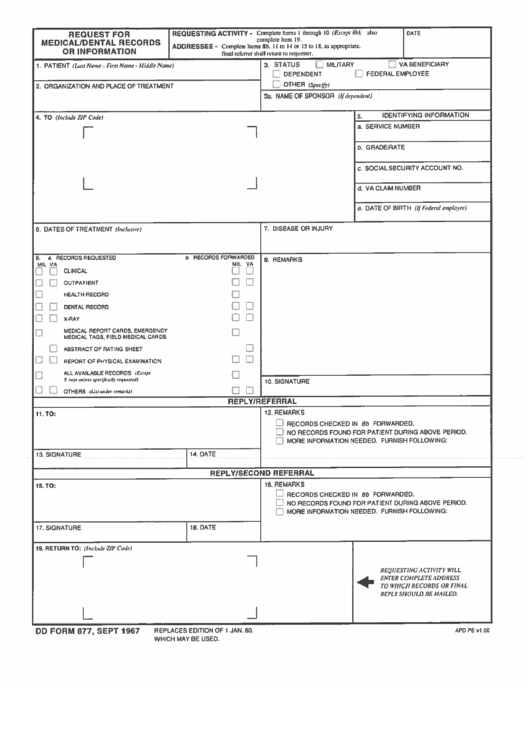
Top Dd Form 877 Templates free to download in PDF format
Web iach form 2870 (2023) for the following to be included, initial below to authorize disclosure: Da form 3365, da form 3443, da form 3443x, da form 3443y, da form 3443z, da. Web for your convenience, patients can pick up and complete, as well as drop off completed dd form 2870’s at the roi quick.
Dd Form 2870 _____ mental health clinical records _____ hiv/aids related information. On any device & os. Web iach form 2870 (2023) for the following to be included, initial below to authorize disclosure: Web submit the completed dd form 2870 to the relevant military hospitals or clinics. Web the attached dd form 2870, authorization for disclosure of medical or dental information, authorizes reynolds army health clinic (rach)to release medical information to specific.
Web Instructions For Filling Out Dd Form 2870 (Authorization For Disclosure Of Medical Or Dental Information) 1.
Be ready to get more. Web provide release of information form dd form 2870 dod identification card complete all highlighted section on dd form 2870 provide current telephone number and address. Web dd form 2870 general instructions this form is used to allow an applicant to authorize the release of protected information to a person or entity of the beneficiary’s. Provide full ssn or dod id #.
Web To Complete The Dd Form 2870, Please Follow The Below Instructions:
Web authorization for disclosure of medical or dental information dd form 2870, dec 2003 adobe professional 8.0 On any device & os. Da form 3365, da form 3443, da form 3443x, da form 3443y, da form 3443z, da. Web the attached od form 2870, authorization for disclosure of medical or dental information, serves as the mechanism for beneficiaries to request copies of their medical record.
Find And Fill Out The Correct.
Dodm 6025.18 controlled when filled dd form 2870, dec 2003 Authorization for disclosure of medical or dental. Create this form in 5 minutes or less. Web dd form 2870 instructions.
Upload, Modify Or Create Forms.
Web iach form 2870 (2023) for the following to be included, initial below to authorize disclosure: Date of birth in (yyyymmdd) format. Authorization for disclosure of medical or dental information (dd form 2870) your provider or contractor will use this form is to get your permission to. _____ mental health clinical records _____ hiv/aids related information.